
Sleep disordered breathing refers to respiratory conditions that cause abnormal breathing patterns during sleep.
The most common types of disordered breathing events are apneas and hypopneas. Apneas involve complete cessation of airflow for 10 seconds or longer, while hypopneas are partial reductions in airflow of at least 30% for 10 seconds or more.
Understanding the key differences between the various forms of apnea and hypopnea is important for proper diagnosis and selecting effective treatment options.
Types of Respiratory Events
Central Apnea
Central apnea involves complete cessation of respiratory effort due to lack of drive from the central nervous system. The brain fails to transmit signals to initiate breathing, resulting in pauses with no chest or abdominal movement.
Central apneas often occur following arousal from sleep and are associated with REM sleep. The pattern of breathing in central apnea is cyclical with ventilatory drive returning periodically. Blood oxygen levels typically drop during the events due to lack of airflow.
Causes of central apnea include heart failure, neurological disorders, opioid medication use, and damage to the respiratory control center in the medulla oblongata.
The condition can also occur in otherwise healthy individuals, especially in REM sleep. Individuals with central apnea have unstable ventilatory control and can experience hypercapnia due to repeated events.
Obstructive Apnea
Obstructive apnea involves physical collapse of the upper airway during inspiration resulting in blocked airflow despite ongoing respiratory effort. The airway muscles relax during sleep causing soft tissues like the tongue and throat to vibrate and intermittently obstruct.
Breathing attempts continue against the blocked airway resulting in loud snoring or gasping when the airway reopens.
Obstructive events can occur in any sleep stage but are most frequent in REM sleep when muscle relaxation is greatest. Oxygen saturation drops with each event and can remain low between apneas due to continued respiratory effort against obstructions.
Obstructive apnea is associated with obesity as excess fat deposits increase airway narrowing. Other risk factors include enlarged tonsils, receding chin, and nasal congestion.
Hypopnea
A hypopnea refers to an abnormal reduction in airflow of at least 30% for 10 seconds or longer accompanied by oxygen desaturation or arousal. By definition, hypopneas involve partial rather than complete obstruction of breathing.
The upper airway narrows but some airflow continues, resulting in shallow breaths. Like obstructive apneas, hypopneas occur when airway muscles relax during sleep, often indicated by snoring.
Hypopneas can precede or follow apneic events as the airway alternates between partial and complete collapse.
The frequency of arousals and sleep fragmentation seen with hypopneas can significantly impact sleep quality and architecture. Hypopneas are also associated with drops in oxygen saturation. Risk factors include obesity, nasal obstruction, and sedative use.
Key Differences
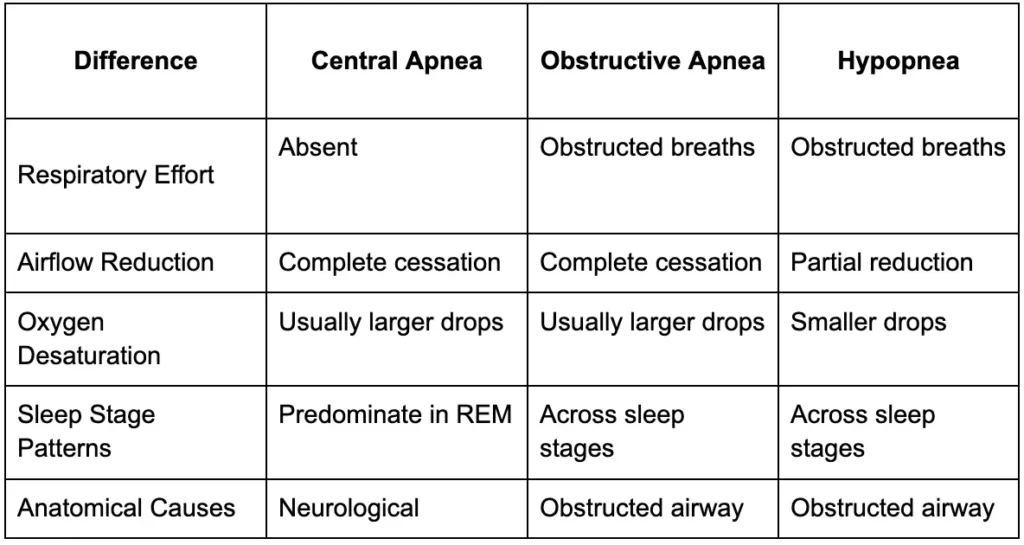
The key differences between these respiratory events include:
- Respiratory effort – absent in central apnea vs obstructed breaths in obstructive apnea and hypopnea
- Airflow reduction – complete cessation in apneas vs partial reduction in hypopneas
- Oxygen desaturation – central and obstructive apneas usually have larger drops compared to hypopneas
- Sleep stage patterns – central apneas predominate in REM while obstructive events are across sleep stages
- Anatomical causes – central is neurological vs obstructed airway in obstructive forms
Measuring and Identifying the Events
The apnea-hypopnea index (AHI) is used to quantify the severity of sleep disordered breathing based on the average number of apneic and hypopneic events per hour of sleep.
AHI is determined through polysomnography, an overnight sleep study that monitors brain waves, oxygen levels, breathing, and other physiological parameters.
Repeated arousals from sleep are also indicative of breathing events. The number of arousals and their association with respiratory effort can help distinguish central from obstructive patterns.
Symptoms like frequent loud snoring, gasping during sleep, and excessive daytime sleepiness may also help identify obstructive disorders. Accurate identification of the specific type of respiratory event is crucial for selecting appropriate treatment approaches.
Diagnosing Sleep Apnea and Hypopnea
Accurate diagnosis is essential for determining the type of disordered breathing and guiding appropriate treatment. Polysomnography conducted during an overnight sleep study remains the gold standard for assessing sleep apnea and hypopnea. This comprehensive test monitors brain waves, heart rate, breathing patterns, and oxygen saturation.
The data gathered calculates the apnea-hypopnea index (AHI) to quantify severity based on the number of events per hour. An AHI of 5-15 is mild, 15-30 is moderate, and over 30 is severe.
Polysomnography also detects subtle respiratory effort-related arousals indicative of airway resistance. Sleep clinicians can identify central vs obstructive apnea based on the presence or absence of breathing efforts.
Symptoms such as excessive daytime sleepiness, loud snoring, and observed breathing pauses during sleep help identify those at risk needing further diagnostic testing. Portable at-home sleep tests that monitor oxygen saturation, breathing, and heart rate are sometimes used for screening prior to in-lab polysomnography.
Impacts on Health
Frequent apneas and hypopneas can significantly impact health, sleep quality, and daytime functioning. The intermittent drops in oxygen and increased carbon dioxide caused by these events stress the cardiovascular system. Sleep fragmentation from repeated arousals prevents restorative deeper stages of sleep.
These factors increase risk for hypertension, heart disease, stroke, cognitive impairment, and metabolic disorders. Assessing the type and severity of disordered breathing is important for mitigating long-term health consequences.
Treatment Options
Treatment options for sleep disordered breathing include:
Positive Airway Pressure (PAP) Devices
PAP delivers pressurized air through a mask to splint the airway open during sleep. Continuous Positive Airway Pressure (CPAP) provides a constant pressure while Bilevel PAP delivers a higher pressure during inhalation and lower during exhalation.
Auto-titrating PAP devices adjust pressure based on respiratory effort. PAP is highly effective for obstructive apnea and often first-line due to being non-invasive. However, managing the airway mechanically with PAP targeting the symptoms may be insufficient to fully treat more complex central apnea causes.
NightLase®
Through proprietary light-guided tissue toning technology, patients can now experience non-invasive relief from snoring and sleep apnea like never before – with NightLase®.
By gently stimulating collagen contraction in key oral areas, NightLase® delicately lifts and supports the tissues responsible for disruptive sounds and breathing interruptions. The result? Vastly improved quality of sleep through reduced vibrations and a clearer airway.
Best of all, the NightLase® process involves zero pain or downtime. Most patients complete the simple, in-office sessions while fully awake. And long-lasting effects are achievable with just three to five treatments over six to ten weeks – far exceeding traditional options.
NightLase® medical providers and dentists also appreciate the program’s ease of use. No laser certification or anesthesia is needed to provide patients this life-changing therapy.
Oral Appliances
Custom-made oral appliances such as mandibular advancement devices work by advancing the jaw and tongue forward to enlarge the airway.
They can be an alternative for mild-moderate obstructive apnea when CPAP is not tolerated. Success depends on the apnea type and requires follow-up to ensure proper fit as the jaw changes over time.
Surgical Options
For obstructive sleep apnea caused by tongue base collapse or tonsillar hypertrophy, surgical treatments like uvulopalatopharyngoplasty (UPPP) or tonsillectomy may improve symptoms.
However, surgery alone often does not resolve obstructive apnea and may require follow-up PAP to fully address sleep disordered breathing.
Supplemental Oxygen
Nocturnal oxygen therapy can potentially treat central sleep apnea linked to hypoxemia by preventing ventilation responses to desaturation. However, identifying and managing underlying triggers such as heart failure is also important.
The most effective treatment strategy considers accurate disease phenotyping along with patient lifestyle factors and preferences to select targeted, multi-disciplinary therapies personalized to the individual.
Managing Sleep Apnea and Hypopnea with Lifestyle Changes
Alongside medical treatment, lifestyle modifications can help manage sleep apnea and hypopnea. Losing weight through diet and exercise reduces fat deposits around airway tissues associated with obstructive breathing events.
Avoiding alcohol and sedatives improves airway muscle tone during sleep. Positional therapy with specially designed pillows prevents sleeping on the back which exacerbates airway collapse.
Practicing good sleep hygiene with a consistent sleep schedule, comfortable bedding, and noise/light control promotes deeper, more restorative sleep.
Ongoing positive airway pressure (PAP) device use greatly reduces respiratory events for patients with moderate to severe sleep apnea. Oral appliance use, nasal dilators, and certain over-the-counter snoring aids also provide symptomatic improvement for mild cases.
Health Implications of Untreated Sleep Apnea and Hypopnea
Leaving moderate to severe sleep apnea and hypopnea untreated can result in serious cardiovascular, metabolic, and neurocognitive consequences.
Recurrent oxygen desaturation and arousals cause physiological stress. Chronic fragmentation of deep sleep stages impairs restorative functions.
These effects increase risks for hypertension, arrhythmias, stroke, heart failure, diabetes, obesity, and mood disorders.
Cognitive impairment and excessive daytime sleepiness from poor sleep quality impacts work performance, driving safety, and quality of life. Screening and diagnosis are critical first steps to mitigating long-term health risks through proper management of sleep disordered breathing.
Conclusion
Central apnea, obstructive apnea, and hypopnea share similarities but have distinct differences in terms of respiratory effort, airflow reduction, oxygen impacts, sleep stage patterns, and anatomical causes.
Accurately measuring and identifying these respiratory disturbances through polysomnography and assessment of symptoms is crucial for developing an effective treatment plan. Treating sleep disordered breathing can improve health outcomes and quality of life.







